


Do You Need A Stent To Treat Your Heart Disease?
The decision to stent a coronary artery used to be simple. Now, it is less so.

One of the most common questions I get is, “Do I need a stent to treat my heart disease?”
Typically, several of this person’s friends have had stents, so it seems natural to ask.
First, we must understand what a stent is and why it is used.
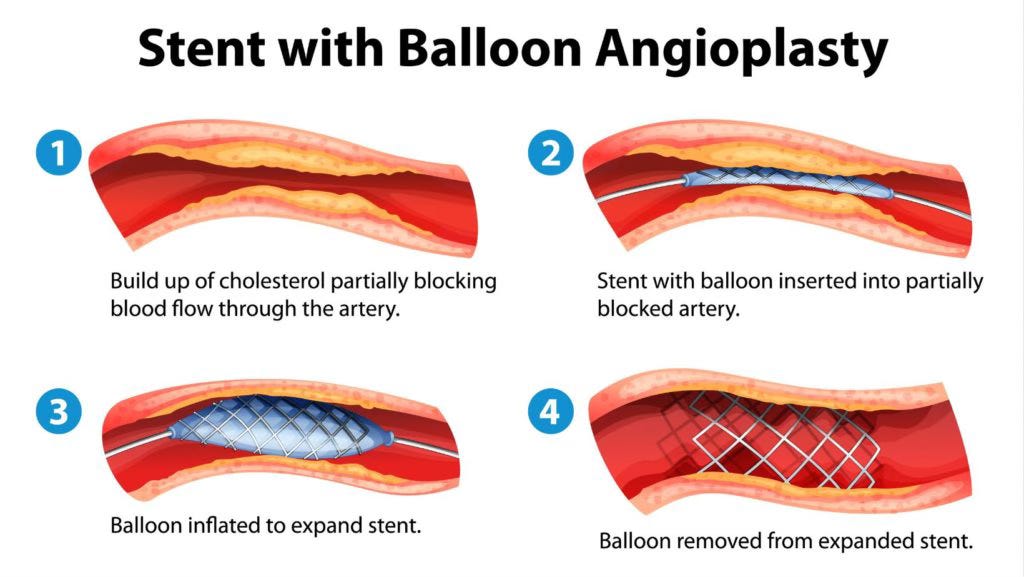
A stent is a metal scaffold deployed in a coronary artery that has reduced flow in that artery to restore flow.
Keep reading with a 7-day free trial
Subscribe to Dr Paddy Barrett to keep reading this post and get 7 days of free access to the full post archives.