


The Data For Weight Loss Medications Just Keeps Pouring In.
Why the weight loss medications known as incretins are turning point in medical history.

“There are decades where nothing happens; and there are weeks where decades happen.”
Vladimir Ilyich Lenin.
It always feels strange to quote Lenin, but when it comes to weight loss medications, it is hard not to feel that decades are happening right before our eyes.
For over 50 years, rates of those who are overweight or obese have been rising rapidly.
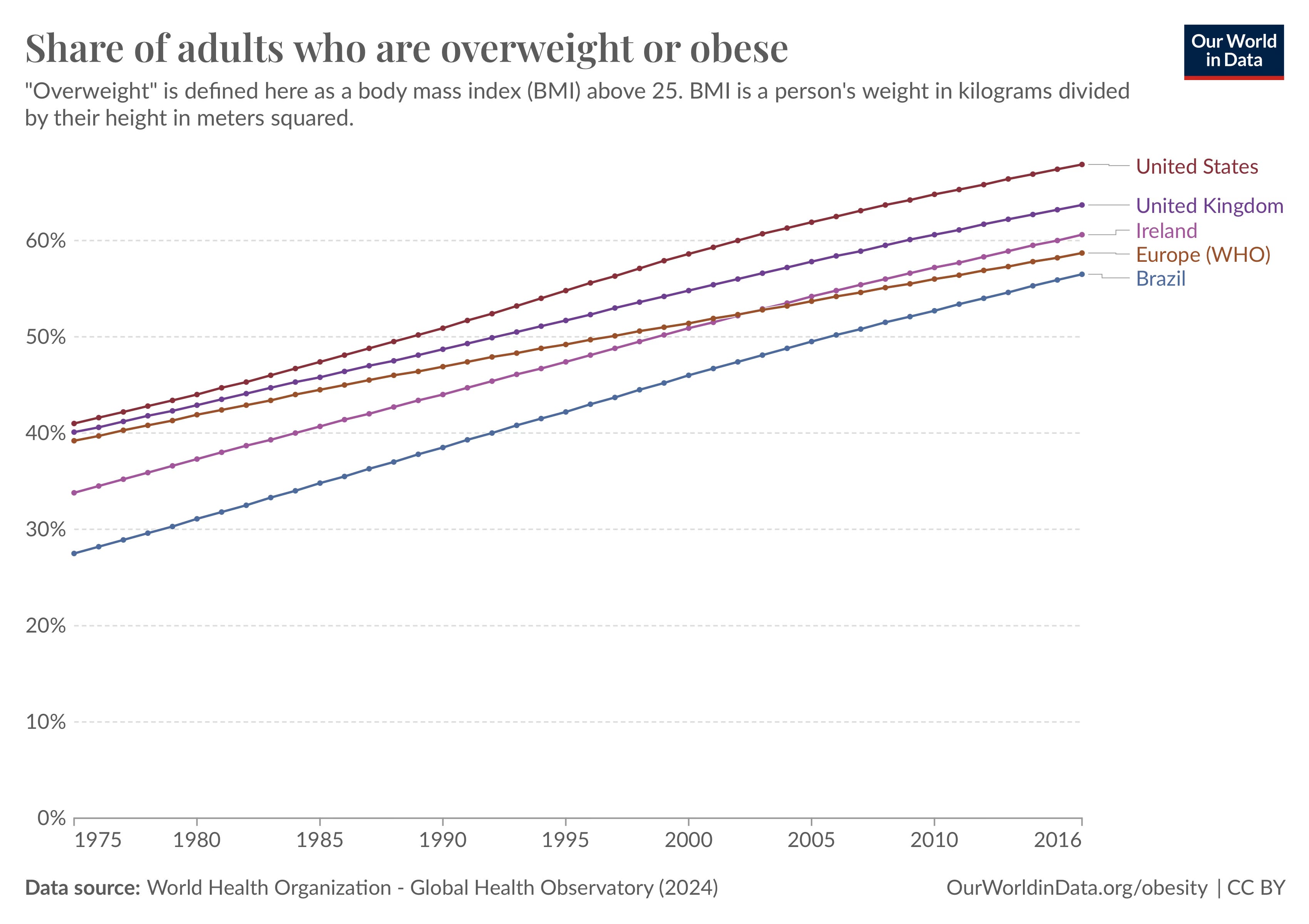
Th…
Keep reading with a 7-day free trial
Subscribe to Dr Paddy Barrett to keep reading this post and get 7 days of free access to the full post archives.