

To Understand Heart Disease, You Need To Understand This.
To Understand Heart Disease, You Need To Understand This.
There is a big difference between the risk factors for heart disease and the disease itself.

Heart disease does not kill people.
Heart attacks do.
Appreciating this distinction is critical to understanding heart disease.
Heart disease is the presence of plaque or atherosclerosis in the coronary arteries.
(Heart disease can, of course, refer to many other heart-related conditions, but in general, the terms heart disease and coronary artery disease or atherosclerosis are typically used interchangeably)
A heart attack occurs when plaque ruptures in the artery, forming a clot that blocks blood flow down the artery, and the heart muscle dies.

Over a long enough time horizon, pretty much everyone will develop a significant amount of plaque and have a heart attack.
This, of course, could be 200 years of age for some people.
So, over the course of an average lifespan, it is unlikely to be an issue for them.
The key takeaway from this should be that to minimise the chances of dying from heart disease; you need to minimise the amount of plaque buildup over your lifetime.
We have very strong evidence to support the idea that the more plaque you have, the greater your risk of a heart attack1.
We also know the reason healthy centenarians do not die from heart disease at a very young age is that they do not develop significant heart disease until very late in life.
On average, they develop serious heart disease about 20 to 25 years later than everyone else2.

While the healthy centenarians have a good portion of genetic luck, they provide an important model that we can copy.
Risk. Disease. Event.
We want to prevent the ‘Event’ that causes our death. In this instance, a heart attack.
The ‘Event’ is caused by the ‘Disease’, atherosclerosis in this instance.
But we know that most people get the ‘Disease’ at some point.
The question is, can we mere mortals get the ‘Disease’ many years later than we normally would so we can emulate our healthy centenarian population?
The answer is yes.
Can we push it out by 20 to 25 years?
Probably not.
Can we push it out by ten or more years?
Probably yes!
But how?
To get heart disease as late as possible in life you need to minimise the amount and severity of risk factors you are exposed to over your lifetime.
This is where ‘Risk Factors’ come into play.
Because before the step of ‘Disease’ comes ‘Risk Factors’.

If we aggressively manage the ‘Risk Factors’ for as long as possible in life, we delay the onset of ‘Disease’.
We, therefore, decrease the probability of an ‘Event’ (Heart Attack) and, therefore, the chances of dying (early).
But does this approach work?
Yes.
If you take young people and look at whether they have gotten most, if not all, of their risk factors in check and compare them to those who do not have their risk factors in check, you see a massive difference in risk over the following 30 years.
For those who get seven risk factors in check, their risk of dying from heart disease decreases by 93%3.
If the gravity of that last sentence didn’t hit you like a ton of bricks, I suggest you go back and read it again.
And remember, this is a 93% decrease in the condition most likely to kill you!
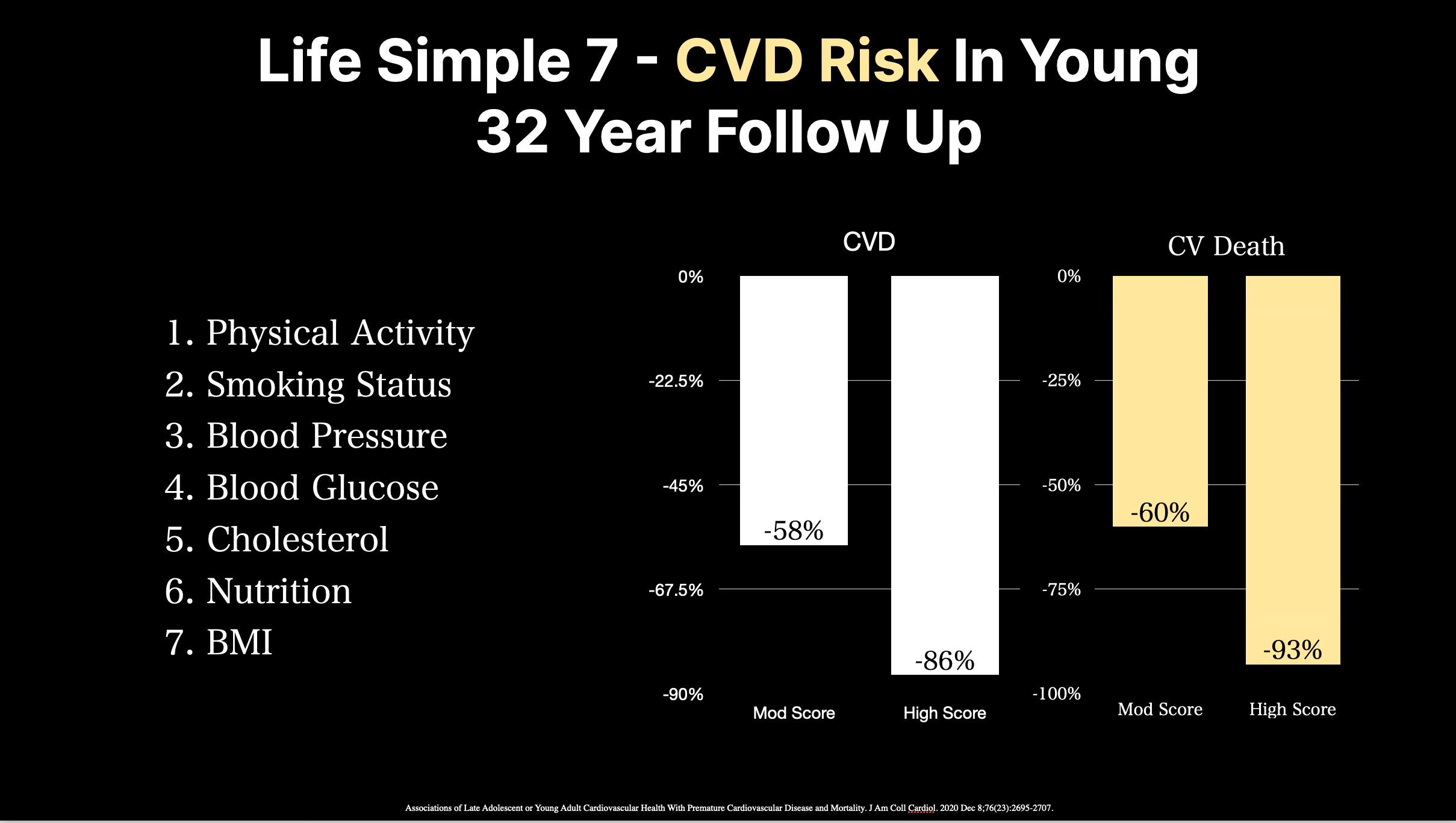
Even getting only some of these risk factors in check decreases the risk of dying from heart disease by 60%.
But remember, these people started early in life.
And we know that heart disease starts to appear early in life so the earlier you address risk factors the better.
This is why waiting until you are 50 years of age to start taking heart disease seriously is just a bad idea.
You will have missed a considerable window of time to make a difference.
You really do want to start setting the odds in your favour early in life.
But what if you DID wait until later in life?
If you are in your 50s as a male or female, you almost certainly have early-stage atherosclerosis.
The question is if that ‘early stage’ atherosclerosis is very early stage fibroatheroma or the early phases of advanced atherosclerosis with calcification of that plaque.
Once calcification appears in coronary atherosclerosis, it is a late-stage feature.
If it is present in small amounts, it is in the early days of that process and confers only a small degree of risk in the near term.
Lifetime risk is another issue.
But if you are in your 50s and want to get a snapshot ‘IF’ the risk factors you have had to date have translated into advanced plaque, you can look directly for that calcification with a cardiac CT.
In the setting of a CT CAC of 0 and or no evidence of calcified or non-calcified plaque on these scans, it means two things.
You have no evidence of ‘Advanced’ plaque, but you still likely have early-stage plaque that is not visible because of the scan's limitations.
Your risk of an ‘Event’ such as a heart attack is very low over the near term. Probably less than 2%. When I say near term, I mean ten years.
When I meet someone in their 50s who is starting to focus on decreasing their lifetime cardiovascular risk, a cardiac CT scan can be a very useful tool to ‘stage’ where someone is on their journey.
However, the optimal strategy is always to address risk factors as early as possible in life, which usually means a more focused approach to lifestyle interventions.
But sometimes, medications.
The key thing to remember, however, is that you always need to think of this process in stages.
Risk factors: High LDL-C, High Blood Pressure, Excess Weight, Insulin Resistance, etc.
Disease: Coronary Atherosclerosis.
Event: Heart Attack.
When attempting to address these issues you always need to know where you are on this journey and that addressing risk factors early in life rather than waiting for disease is always the best long term strategy.
I have yet to meet someone serious about reducing lifetime cardiovascular risk that didn’t regret not starting to address risk even earlier in life.
But even if you haven’t, there is always a lot you can do to reduce your future risk.
Association of coronary artery calcified plaque with clinical coronary heart disease in the National Heart, Lung, and Blood Institute's Family Heart Study. Am J Cardiol. 2006 Jun 1;97(11):1564-9.
J Gerontol A Biol Sci Med Sci. 2012 Apr;67(4):395-405.
Associations of Late Adolescent or Young Adult Cardiovascular Health With Premature Cardiovascular Disease and Mortality. J Am Coll Cardiol. 2020 Dec 8;76(23):2695-2707.
Thank you. This is ultimately very helpful directionally.
Excellent review. This is why I disagree with the current guidelines on starting statins only if the 10-year risk is higher than a certain number +/—risk factors. It ignores lifetime risk. At age 75, I am glad that I started statins more than 30 years ago for only prevention, not because of a high LDL or risk factor indication. 30 years of lower LDLs, even if the pre-statin LDL was not very high, pushes out the lifetime risk.