
Why Walking Is A Longevity Superpower.
At high levels, walking is linked to an almost 80% reduction in the risk of heart disease.

The single most powerful intervention in preventive cardiology is free, unpatented, and probably already in your shoes.
Patients arrive in my clinic exhausted by the exercise recommendations on social media.
Continuous glucose monitors strapped to people without diabetes.
Wearables telling them their nervous system is underrecovered.
Endless argument about whether they should be doing zone 2 or zone 5, both or neither, and which supplement to layer on top.
They want to know what to fix next.
For most people, the answer is…. Walk more.
It doesn’t sell anything, which is part of why you don’t hear it enough.
Two separate strands of evidence make this hard to argue with.
Start with steps.
A 2023 meta-analysis in the European Journal of Preventive Cardiology pooled seventeen cohorts and 226,889 people. [1]
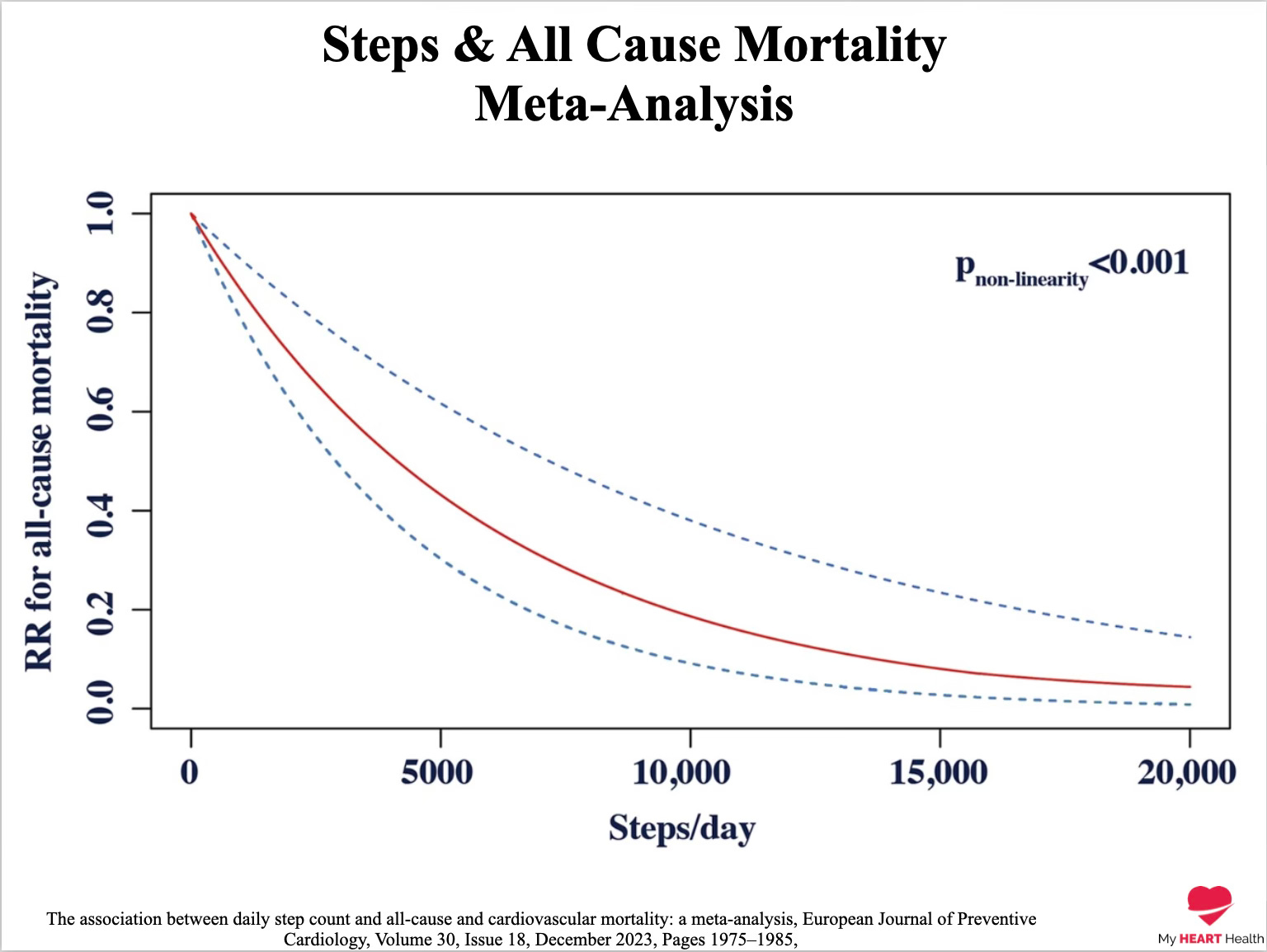
Every additional 1,000 steps a day mapped to a 15% drop in all-cause mortality.
Every additional 500 steps, a 7% drop in cardiovascular death.
The benefit was already detectable at around 4,000 steps a day, well below the 10,000 figure that gets repeated everywhere and that almost nobody can source.
At the most active quartile measured, all-cause mortality risk was roughly two-thirds lower, and cardiovascular mortality risk about three-quarters lower.
The investigators tracked the relationship out to 20,000 steps a day.
The curve never plateaued and never bent the wrong way.
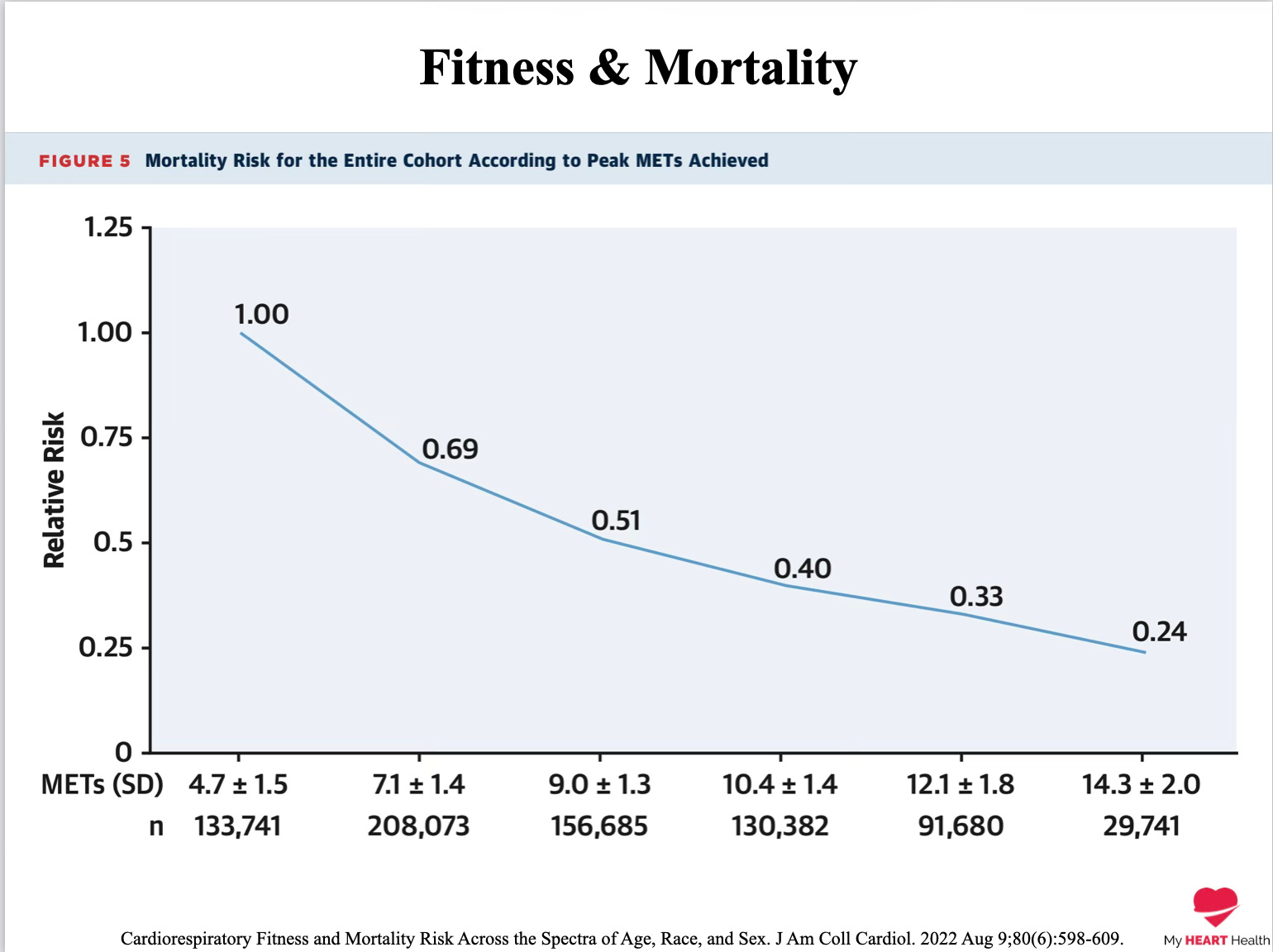
In a Cleveland Clinic cohort of 122,007 people undergoing treadmill testing, the fittest group had an 80% lower adjusted mortality risk than the least fit. [2]
That gap was larger than the increase in mortality associated with smoking, with established coronary artery disease, or with diabetes.
A separate analysis of 750,302 US veterans found the same inverse, graded relationship across men and women, every major ethnic group studied, and into septuagenarians and octogenarians. [4]
No upper limit. No point at which extra fitness stopped paying dividends. [4]
Walking matters. Fitness matters. Neither has a ceiling we have found. [1,2,4]
A distinction worth being careful about, because patients confuse it constantly.
Walking does not dissolve plaque. It will not normalise high cholesterol. It will not undo twenty years of untreated hypertension.
There is no amount of walking or fitness that immunises you from heart disease.
Walking is great, but it isn’t holy water!
Atherosclerosis runs on its own clock, and someone walking 12,000 steps a day on a wrecked lipid panel is still walking toward an event.
What walking does is shift the trajectory of the person carrying the disease.
It lowers the probability of the event early in life.
It hardens you against the comorbidities that pile up in mid and late life.
It buys years of physical independence at the back end.
Lipids and blood pressure determine how aggressive the disease is.
Fitness determines how well you survive it.

The other piece — the one most patients have never been told — is that none of this is fixed.
Most fitness studies measure people once, which makes the whole topic feel deterministic.
As though the card has been dealt at birth. It hasn’t.
A 2023 Journal of the American College of Cardiology paper followed 93,060 people who had two treadmill tests an average of 5.8 years apart. [3]
People whose fitness improved by approximately one MET or more saw their mortality risk fall, regardless of baseline fitness. [3]
People whose fitness declined saw their risk climb, with the effect strongest in those with established cardiovascular disease.
The pattern held in those with and without cardiovascular disease.
The body keeps responding for as long as you keep using it.
If you are sedentary, the first 4,000 extra steps a day will shift your risk profile more than the next 4,000.
The dose-response is nonlinear, with the steepest reduction in mortality at the lower end of the curve. [1]
Start there. And then build in more steps over time.
If you are already active, more still helps.
The curve flattens but it does not turn down. [1,2]
There is no point in this literature at which walking becomes the problem.
If you can occasionally make it harder — a hill, a faster pace, the stairs taken with intent — your VO2 max responds.
And VO2 max is the variable that tracks survival also. [2,4]
You do not need a ring or a watch for any of this. The device is feedback. It is not the intervention.
Walking Helps But Doesn’t Cure.
Walking is not a replacement for medical therapy.
People who need statins, antihypertensives, or treatment for diabetes still need them, and walking adds to those benefits rather than substituting for them.
The mechanisms are different. They stack.
It is not proof of causation. The data are observational, and people who walk more tend to do other things differently too. [1,2,3,4]
The signal is consistent enough across studies, populations, and decades that I act on it clinically — but I won’t pretend that is the same as a randomised trial.
And it doesn’t mean more is always better in every form of exercise. High volumes of vigorous exercise has been associated with atrial fibrillation, coronary artery calcification, myocardial fibrosis, and aortic dilation in some cohorts. [2]
None of that applies to the kind of activity discussed here.
Walking is low intensity. You can knock yourself out with the volume.
Most of what gets framed as longevity advice on social media will not matter in twenty years.
The supplement having a moment. The protocol with the breathless launch. The lab panel screenshot from someone with a podcast and an affiliate code.
Walking will still matter.
It is, as far as we can measure, the closest thing in preventive cardiology to a free intervention with a survival benefit on the same scale as the drugs we work hardest to get our patients to take. [1,2,3,4]
It works in middle age, in old age, and in people who have already had something go wrong. [3,4]
The dose is whatever you can keep doing.
You can almost certainly take more steps tomorrow than you did today.
Start there.

References
Banach M, Lewek J, Surma S, et al. The association between daily step count and all-cause and cardiovascular mortality: a meta-analysis. Eur J Prev Cardiol. 2023;30(18):1975–1985.
Mandsager K, Harb S, Cremer P, Phelan D, Nissen SE, Jaber W. Association of cardiorespiratory fitness with long-term mortality among adults undergoing exercise treadmill testing. JAMA Netw Open. 2018;1(6):e183605.
Kokkinos P, Faselis C, Samuel IBH, et al. Changes in cardiorespiratory fitness and survival in patients with or without cardiovascular disease. J Am Coll Cardiol. 2023;81(12):1137–1147.
Kokkinos P, Faselis C, Samuel IBH, et al. Cardiorespiratory fitness and mortality risk across the spectra of age, race, and sex. J Am Coll Cardiol. 2022;80(6):598–609.