
Cholesterol Lowering Tools
We have so many options to address a major risk factor

Before getting into the details, it is always best to take a step back and frame the problem you are trying to solve.
Cardiovascular disease is the leading cause of death worldwide1.
High cholesterol accounts for over half of the risk of cardiovascular disease in both males and females2.
High cholesterol CAUSES coronary artery disease3.
Individuals with lifelong elevated cholesterol are at a significantly increased risk of cardiovascular disease4.
Individuals with lifelong low cholesterol levels are at a significantly lower risk of cardiovascular disease5.
We have the tools to reduce cholesterol by 85%6.
A lifelong reduction in cholesterol would virtually eliminate the risk of coronary artery disease7.
To significantly reduce the impact of the leading cause of death worldwide, the goal is to have low cholesterol for as long as possible.
How do we do this?
In 2 ways:
Lifestyle
Drug therapy
Lifestyle
High cholesterol is a function of two elements; lifestyle and genetics.
Estimates vary, but about 40 - 50% of high cholesterol is a function of genetic factors8. Although this leaves a significant percentage unexplained, it does not mean that it all relates to lifestyle. Some of it certainly does, but a substantial percentage of that remaining 50% is also likely down to unmeasured genetic or non-modifiable factors.
Poor lifestyle decisions primarily related to nutrition do raise cholesterol levels. Correcting these components should, of course, be the first step to lowering elevated cholesterol levels. But is it likely to get cholesterol levels low enough for adequate lifetime risk reduction?
Improving nutrition can lower cholesterol levels by 20 - 30%, which for many people will make a big difference to the lifetime cardiovascular risk9.
But will it lower cholesterol levels to the point where cardiovascular risk is significantly reduced? In those with very mild cholesterol elevations, it might, but for most people, it won’t, for two reasons.
Firstly, they are unlikely to achieve a cholesterol low enough to reduce their risk substantially. Secondly, the likelihood of adhering to that dietary pattern over a lifetime is often poor. Some can do it, but many more can’t and don’t.
For most people, to attain lifelong reductions in cholesterol to the level that is necessary to minimise risk absolutely, drug therapy will likely be required.
Drug Therapy
Before considering any drug option, the question of safety must be addressed.
Every treatment must be considered in a risk-benefit framework. For most individuals, statin therapy will be the drug of choice to lower cholesterol. Estimates of side effects of statin therapy vary between 0.3 to 33%10. The most common side effects are muscle aches or soreness. When evaluated, 90% of these side effects are unrelated to statin therapy11. This means that the overwhelming majority of patients with side effects while on statin therapy do not have a side effect from the drug but symptoms from alternative causes.
Let me be 100% clear.
I have patients who have had serious side effects from statin therapy. These side effects were very real. They all stopped when the treatment was stopped. So the adverse effect was temporary and reversible.
However, the majority of my patients on statin therapy tolerate them without issue. Most therapies to lower cholesterol are very well tolerated with minimal side effect profiles12. No treatment is without risk, but when it comes to lowering cholesterol, the risk of not lowering it is generally far more than the risk of being on the therapy.
We can lower cholesterol by 85%.
Here’s how.
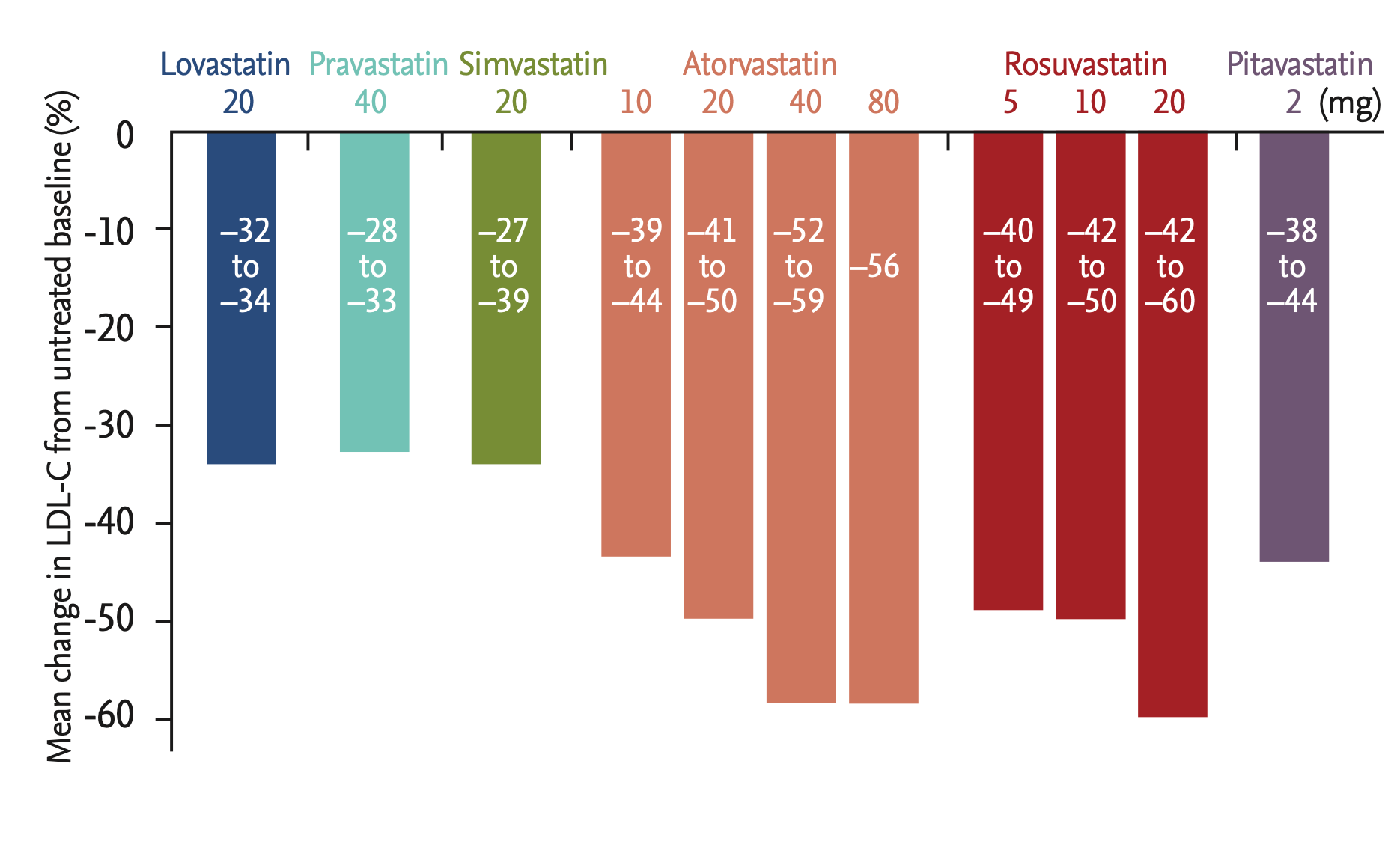
Statins
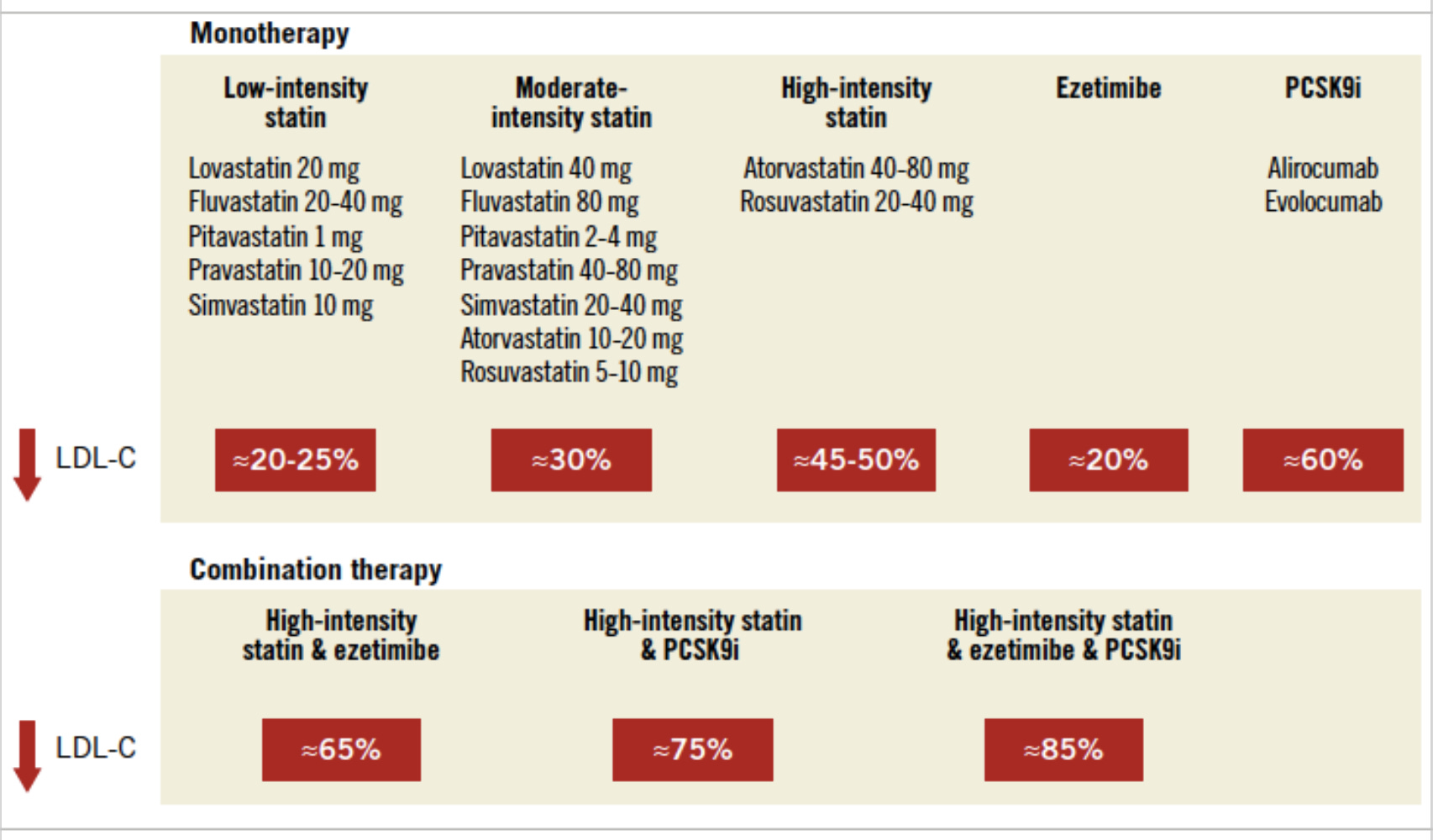
A range of statin therapies are available, usually lowering LDL cholesterol by 20 to 50%. With the average LDL cholesterol in the US at approximately 3.2mmol/l, this level of reduction is most likely to be sufficient for most individuals. Lifelong LDL cholesterol levels of less than 1.4 mmol/l are associated with extremely low cardiovascular event rates13. Statins reduce cholesterol by reducing cholesterol synthesis in the liver and increasing the concentration of LDL receptors in the liver to promote clearance14.
Statin therapy in isolation is likely to be adequate for most people who require drug therapy to lower LDL cholesterol levels.
Ezetimibe
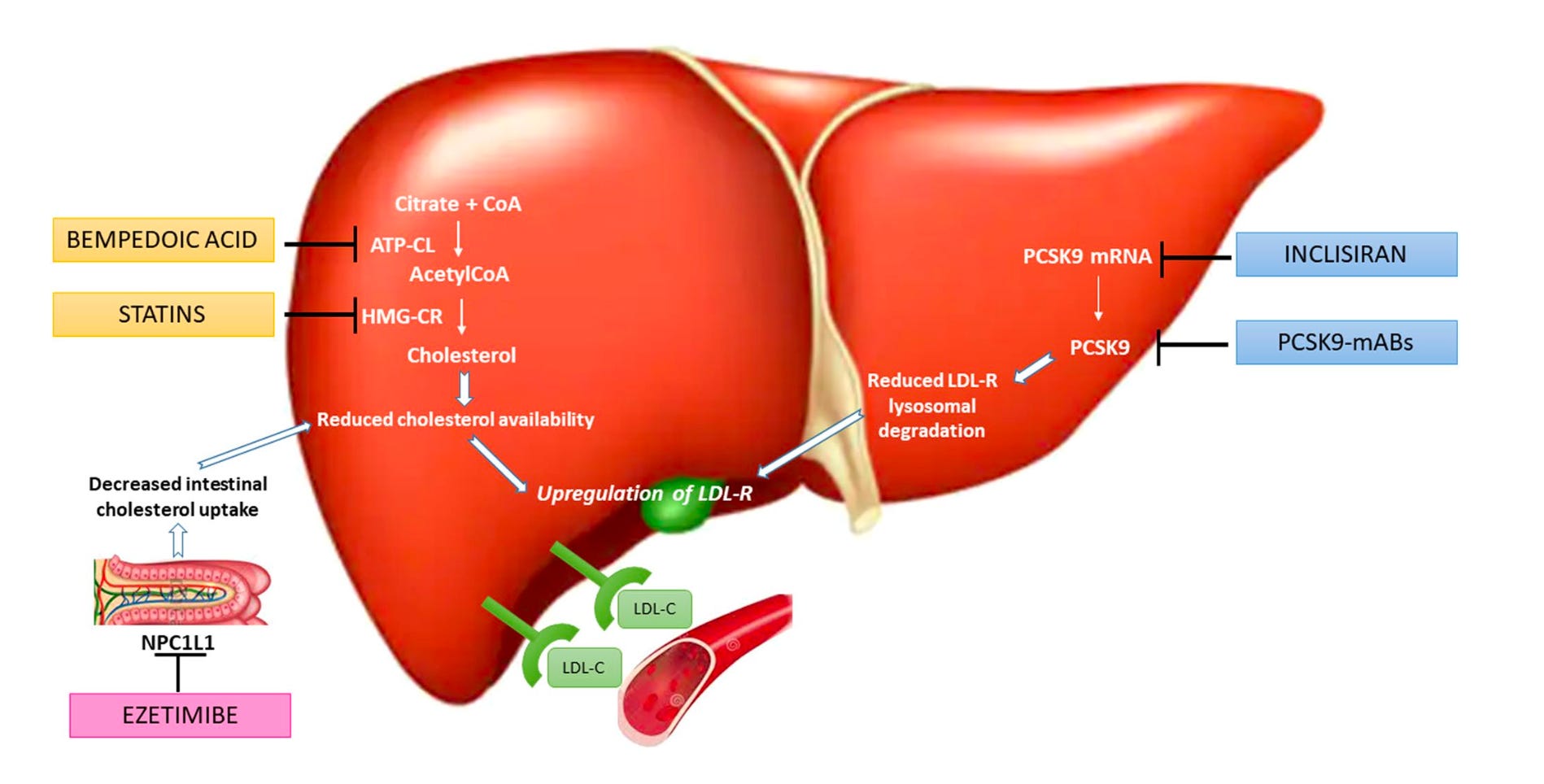
While statins mainly reduce cholesterol production in the liver, ezetimibe reduces cholesterol by increasing absorption from the gastrointestinal system15. This also results in greater numbers of LDL receptors in the liver, resulting in greater clearance of LDL cholesterol from circulation.
Ezetimibe is generally very well tolerated with minimal side effects. It is primarily used in those who are not achieving target LDL cholesterol levels on statin therapy or are intolerant to statin therapy. Ezetimibe typically reduces LDL cholesterol levels by about 20%16.
PCSK9 Inhibitors
Until recently, statin therapy and ezetimibe were the only mainstay therapies available to reduce LDL cholesterol levels.
The next step forward in cholesterol-lowering was the development of PCSK9 inhibitors. These twice-monthly injectable treatments can lower cholesterol levels by about 60% when used in isolation and by 85% when combined with statin and ezetimibe oral therapies.
For individuals with very high cholesterol levels or those with repeated cardiovascular events on maximum oral therapies, these have been a huge step forward. Unfortunately, access to these treatments is often highly restricted because of price constraints and reimbursement by health systems or insurance companies that have to cover most of the cost. This has been a major frustration for those who need these therapies but unfortunately cannot access them because of reimbursement issues.
Bempedoic Acid
The most recent oral LDL cholesterol-lowering therapy is Bempedoic acid which reduces cholesterol similarly to statin therapy but slightly upstream of the point of cholesterol production where statins work.
Although we await outcome data, trials have demonstrated bempedoic acid to be safe and can reduce cholesterol levels by about 18% in addition to that achieved by statin therapy17. This is likely to be a valuable tool for patients not yet at their LDL cholesterol target or who experience adverse effects from other cholesterol-lowering options.
Inclisiran
Acting via the PCSK9 pathway, Inclisiran is a small interfering RNA that is an injectable LDL cholesterol-lowering therapy given every six months after an initial loading phase. Inclisiran can lower LDL cholesterol by approximately 50% in addition to existing therapies18.
When my patients ask me if they will be on statin therapy for life, I say no. You are only going to be on it until something better comes along. The PCSK9 modifying therapies are likely to be that ‘something better’ given their potential to lower LDL cholesterol safely and efficiently.
With the addition of Inclisiran, it is likely now possible to lower LDL cholesterol by even more than 85%.
Could it get any better than that?
Amazingly, yes.
Gene Editing
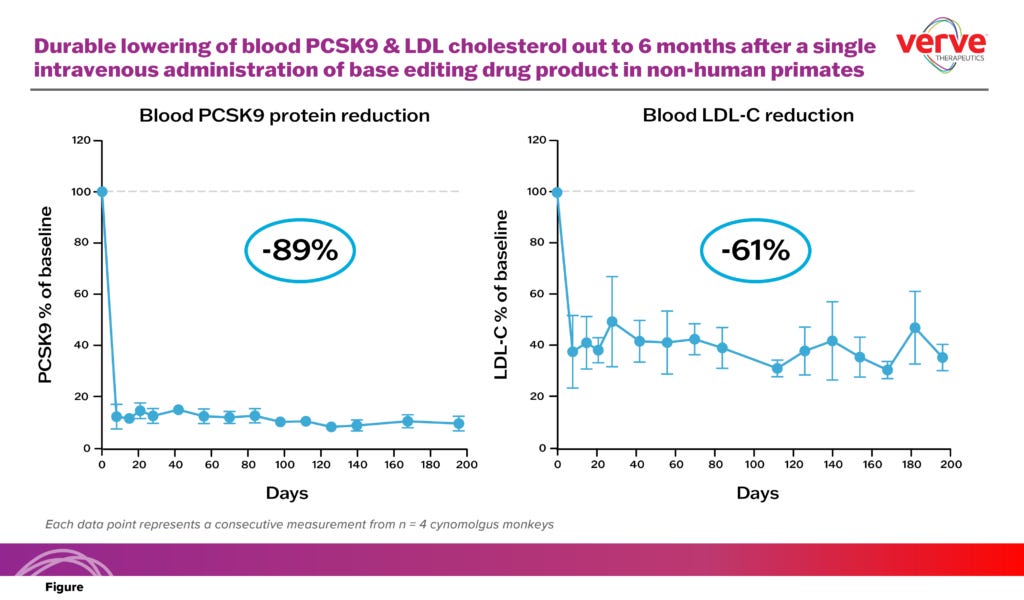
Verve Therapeutics has recently commenced early human trials assessing the safety and effectiveness of using gene editing to turn off the PCSK9 machinery in the liver so as to result in very low LDL cholesterol levels. Initial studies have demonstrated reductions of LDL cholesterol of approximately 60%19. The incredible thing about this approach is that it is a single, once-off treatment for those with genetically high cholesterol20. Although in its early phase, such an approach could herald an era of single-treatment approaches to lifelong low LDL cholesterol.
Given that a major risk factor for coronary artery disease is lifelong elevated cholesterol levels, this new therapy has been dubbed the ‘vaccine’ for high cholesterol.
Cardiovascular disease is the leading cause of death worldwide.
High cholesterol drives approximately 50% of that risk at a population level.
We currently have the tools to dramatically reduce cholesterol levels over a lifetime, and future therapies look even more promising.
The question is how we will use them.
https://ourworldindata.org/causes-of-death
INTERHEART Study Investigators. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004 Sep 11-17;364(9438):937-52.
Low-density lipoproteins cause atherosclerotic cardiovascular disease: pathophysiological, genetic, and therapeutic insights: a consensus statement from the European Atherosclerosis Society Consensus Panel, European Heart Journal, Volume 41, Issue 24, 21 June 2020, Pages 2313–2330
Impact of Lipids on Cardiovascular Health: JACC Health Promotion Series. J Am Coll Cardiol. 2018 Sep 4;72(10):1141-1156.
Sequence variations in PCSK9, low LDL, and protection against coronary heart disease. N Engl J Med. 2006 Mar 23;354(12):1264-72.
2022: The Year in Cardiovascular Disease – The Year of Upfront Lipid Lowering Combination Therapy. Archives of Medical Science. 2022;18(6).
High prevalence of coronary atherosclerosis in asymptomatic teenagers and young adults: evidence from intravascular ultrasound. Circulation. 2001 Jun 5;103(22):2705-10.
Genetics, Lifestyle, and Low-Density Lipoprotein Cholesterol in Young and Apparently Healthy Women. Circulation. 2018 Feb 20;137(8):820-831.
Effects of a Portfolio-Mediterranean Diet and a Mediterranean Diet with or without a Sterol-Enriched Yogurt in Individuals with Hypercholesterolemia. Endocrinol Metab (Seoul). 2020 Jun;35(2):298-307.
https://www.acc.org/latest-in-cardiology/articles/2018/04/09/13/25/assessing-severity-of-statin-side-effects
Cholesterol Treatment Trialists' Collaboration. Effect of statin therapy on muscle symptoms: an individual participant data meta-analysis of large-scale, randomised, double-blind trials. Lancet. 2022 Sep 10;400(10355):832-845.
ESC Scientific Document Group, 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS), European Heart Journal, Volume 41, Issue 1, 1 January 2020, Pages 111–188,
Sequence variations in PCSK9, low LDL, and protection against coronary heart disease. N Engl J Med. 2006 Mar 23;354(12):1264-72.
Statins: mechanism of action and effects. J Cell Mol Med. 2001 Oct-Dec;5(4):378-87.
Perspectives in cholesterol-lowering therapy: the role of ezetimibe, a new selective inhibitor of intestinal cholesterol absorption. Circulation. 2003 Jul 1;107(25):3124-8.
Coronary Computed Tomography Angiography From Clinical Uses to Emerging Technologies: JACC State-of-the-Art Reviews. JACC Vol. 76 No. 10
CLEAR Harmony Trial. Safety and Efficacy of Bempedoic Acid to Reduce LDL Cholesterol. N Engl J Med. 2019 Mar 14;380(11):1022-1032.
ORION-10 and ORION-11 Investigators. Two Phase 3 Trials of Inclisiran in Patients with Elevated LDL Cholesterol. N Engl J Med. 2020 Apr 16;382(16):1507-1519.
https://www.vervetx.com/press-releases/verve-therapeutics-announces-data-demonstrating-durable-ldl-cholesterol-lowering-after-a-one-time-gene-editing-treatment-in-non-human-primates/
https://ir.vervetx.com/news-releases/news-release-details/verve-therapeutics-doses-first-human-investigational-vivo-base
Hi. It would be interesting to hear your take on OTC supplements that can reduce LDL. For example, Plant Sterols and Stanols, Red Yeast Rice extract, and Lecithin Granules. I’ve heard (and witnessed personally, n-=1 I know ) reductions by 75%.
Substack used to be known for its challenging posts. Seems it was too successful as the narrative peddlers are moving in… no doubt encouraged by the Twitter rejects yodelling their psychosis to each other.