
Why Waiting Until Age 50 To Address Risk Factors For Heart Disease Is Too Late.
Why managing cardiovascular risk factors much earlier in life is key.

Most people only start to worry about cardiovascular risk later in life.
This is a bad idea.
Here’s why.
When you look at the risk of having a heart attack, it is true that the older you are, the greater the odds of having a heart attack1.
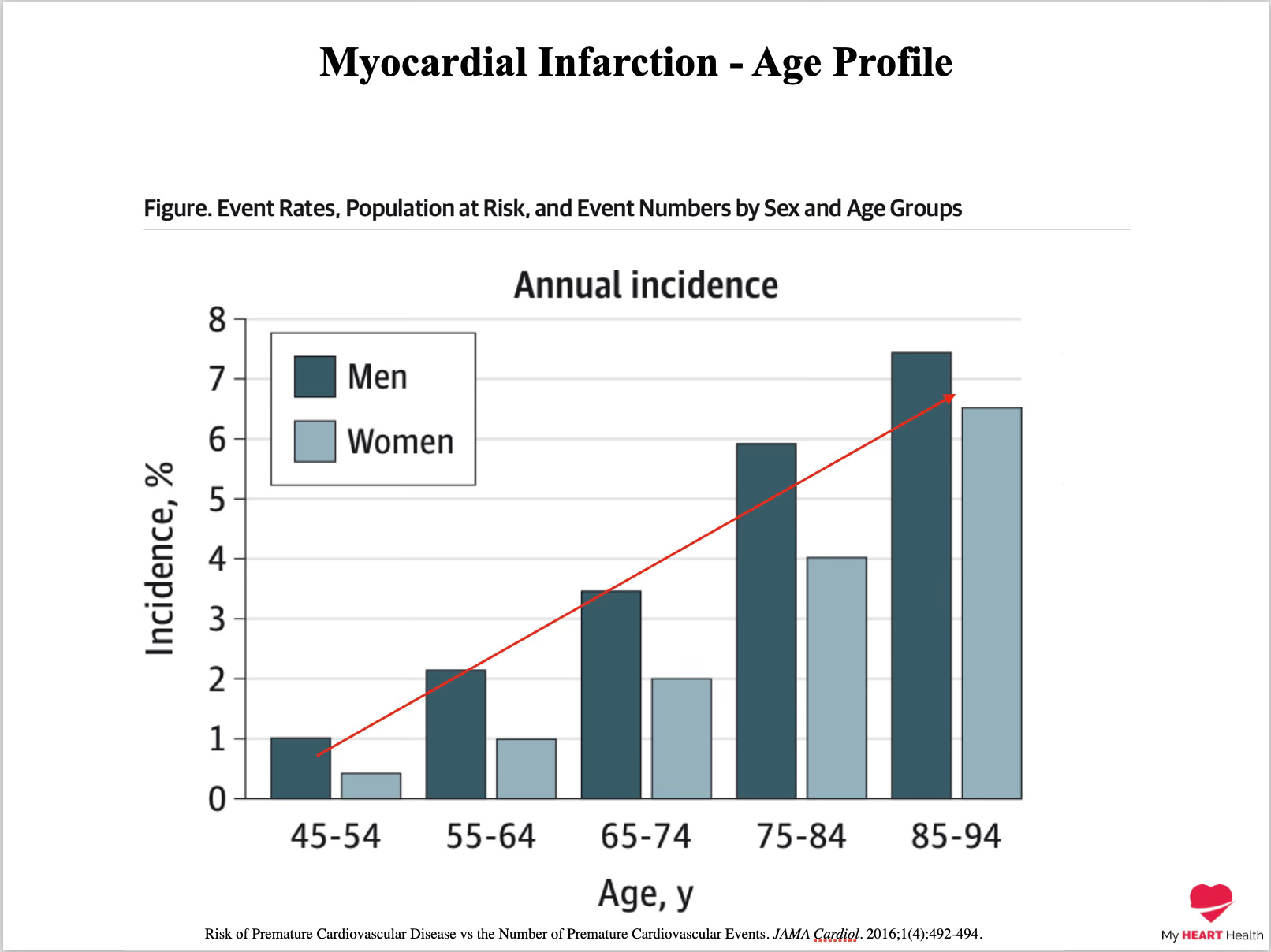
So far, so good.
But this graph is very misleading.
While only 1-2% of those having a heart attack are less than 65 y…
Keep reading with a 7-day free trial
Subscribe to Dr Paddy Barrett to keep reading this post and get 7 days of free access to the full post archives.